
Diagnosis of Fabry disease
Last updated July 29, 2024, by Lindsey Shapiro, PhD
 Fact-checked by Ana de Barros, PhD
Fact-checked by Ana de Barros, PhD
There are a number of tests that might be used to help reach a diagnosis of Fabry disease, a condition marked by deficient alpha-galactosidase A (alpha-Gal A) enzyme activity due to mutations in the GLA gene.
Genetic and enzyme tests, which look for the underlying cause of Fabry disease, are the most definitive ways to establish the presence of the rare inherited disorder. But other tests may be conducted to assess specific disease complications or rule out other conditions.
Due to its progressive nature, it is important for clinicians to make a Fabry disease diagnosis as soon as possible. This enables patients to start on treatments that can slow or prevent the accumulation of life-threatening organ damage.
However, because this disease is a rare genetic disorder, many Fabry patients experience substantial delays before a diagnosis is reached.
The importance of an early diagnosis
In Fabry, mutations in the GLA gene cause patients to have little to no functional alpha-Gal A enzyme, which is needed to break down fatty molecules such as globotriaosylceramide (Gb3) and lyso-Gb3 inside cells. As a result, these substances toxically accumulate over time and cause progressive organ damage and other Fabry disease symptoms.
There are several approved treatments for Fabry disease, namely enzyme replacement therapy and chaperone therapy, that help to lower Gb3 levels and slow the progression of disease-related damage.
But the earliest possible start to Fabry disease treatment is critical for easing discomfort and making daily life easier, as well as for delaying or preventing more serious complications for as long as possible. Thus, an early diagnosis that allows for prompt treatment soon after symptoms emerge could help prolong Fabry disease life expectancy.
However, Fabry disease is a rare condition, and might not be easily recognized by healthcare providers. Some of its early symptoms, such as gastrointestinal issues or pain, may be nonspecific and confused with symptoms from other conditions.
It’s estimated that patients wait an average of 15 years from when their symptoms first appear to when they get a definitive Fabry disease diagnosis, during which damage accumulates in the body’s organs.
It is therefore essential that physicians learn to recognize the signs of Fabry disease and that patients talk with their doctors as soon as they start noticing symptoms or if there’s a family history of the condition.
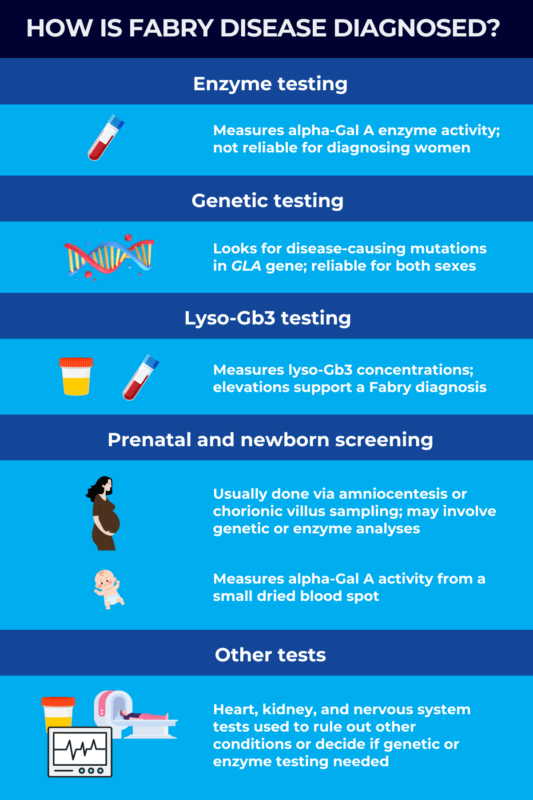
How is Fabry disease diagnosed?
Fabry disease testing may involve a range of different evaluations, including physical exams and blood tests. When a person is first being checked for Fabry disease, their doctor will likely conduct a comprehensive physical exam and review the person’s medical history.
The symptoms of Fabry disease are highly variable, especially for female patients, but some early signs may include:
- nerve-related pain, especially in the hands and feet
- starburst pattern of cloudy areas on the surface layer of the eye (corneal opacity), which is only detected via a special test at the eye doctor
- a clustered skin rash called angiokeratoma
- heat intolerance or reduced/absent sweating.
Because Fabry disease is inherited, a family history of the condition is also a key factor that helps doctors consider the possibility of Fabry disease.
Although numerous medical specialists may suspect Fabry disease based on their respective areas of expertise, a definitive diagnosis is usually made by specialists such as nephrologists (kidney doctors), geneticists, cardiologists, and gastroenterologists. These healthcare professionals conduct a series of diagnostic tests to conclusively identify the presence of Fabry disease.
Enzyme tests
An enzyme test to measure alpha-Gal A activity levels can help to diagnose Fabry disease in certain patients. This test is usually conducted using a small blood sample (dried or liquid), but alpha-Gal A activity can also be measured in cells or tissue.
Any result showing alpha-Gal A activity at 1% of normal or lower — meaning that alpha-Gal A activity is essentially absent — is highly indicative of Fabry and can be used to confirm a Fabry disease diagnosis.
These low activity levels are typically observed in male patients with classic Fabry disease, where symptoms appear earlier in life and are more severe. In males with the milder late-onset Fabry disease, alpha-Gal A levels are often above 1% but are still lower than normal. Subsequent genetic testing may support a diagnosis for these patients.
In females, alpha-Gal A activity is highly variable, with some having normal or near-normal levels. As such, an enzyme test is not enough for a definitive Fabry diagnosis in female patients and genetic testing will be required to diagnose the disease.
Genetic testing
Mutations in the GLA gene are the only known Fabry disease cause, so genetic testing to look for a disease-causing mutation is the most reliable Fabry disease test for all patients.
Fabry disease genetic testing, which can be performed on a small blood or saliva sample, is recommended for any person with a confirmed or suspected Fabry diagnosis.
For male patients already diagnosed with enzyme testing, genetic testing can identify the disease-causing mutation to guide treatment decisions. For female patients, genetic testing is the only way to accurately establish a diagnosis.
Not all mutations in GLA will cause disease. Once a mutation is identified with genetic testing, a person’s doctors may do some research or perform other clinical tests to decide if the mutation is likely disease-causing, especially if a person does not have any symptoms or family history.
Once a person is diagnosed with Fabry disease via genetic testing, other members of their family might also be tested to see if they have the same mutation. This can help establish an early diagnosis and treatment or monitoring plan for affected patients before significant symptoms have started to accumulate. It can also help affected family members make family planning choices.
Lyso-Gb3 tests
While enzyme and genetic testing are the main ways of identifying Fabry in the clinic, blood tests to look for the presence of the fatty substances that accumulate when alpha-Gal A is lacking are another way to support a diagnosis.
Doctors can measure the lyso-Gb3 concentration in blood, skin cells, or urine as an indicator of Fabry disease in both male and female patients, as the biomarker will often be elevated relative to healthy people.
This Fabry disease blood test may be especially useful for identifying Fabry disease in cases where the diagnosis is more difficult, such as in female patients who don’t have symptoms, or in patients with newly-identified GLA mutations whose clinical significance is not established. This test may also be used to monitor disease progression in diagnosed patients.
Prenatal testing and newborn screening
While most Fabry disease diagnoses happen later in life, when a person experiences symptoms or has had a family member diagnosed, there are screening tests that can look for Fabry disease in an unborn fetus or an asymptomatic newborn.
Women with Fabry disease can undergo prenatal testing to check if their unborn fetus will be affected by the condition. There are two different procedures that may be used to obtain samples from the fetus to perform prenatal testing: amniocentesis or chorionic villus sampling (CVS).
In amniocentesis, a small sample of the fluid that surrounds the baby in the placenta is removed, while CVS involves directly taking cells of the placenta. These samples may then be tested for GLA mutations or alpha-Gal A enzyme activity.
Some states have newborn screening programs that test for Fabry disease and related disorders in all newborn babies while they’re still at the hospital. Doctors will take a tiny blood sample from the infant via a heel prick and test it for alpha-Gal A enzyme activity. If alpha-Gal A activity is lower than normal, it does not mean that a baby definitely has Fabry disease, but additional screening tests may be required.
Other tests
During the diagnostic process, patients may undergo other clinical tests to look at the health of their organs, including the heart, kidney, and nervous system, which are particularly affected in Fabry.
Possible tests include:
- echocardiograms and electrocardiograms, two heart tests that create images of the heart and measure its electrical activity, respectively
- brain and heart MRI scans
- tests to detect protein or blood in the urine
- blood tests to establish kidney function.
These tests may help rule out Fabry disease differential diagnoses, and aid doctors in honing in on the need for Fabry genetic or enzyme testing.
After a Fabry diagnosis is established, these tests may also be used to help doctors understand a patient’s disease progression and to develop an optimal care plan.
Why is Fabry sometimes missed in women and children?
The GLA gene resides on the X chromosome, one of the two types of sex chromosomes. Only one mutated copy of the gene is needed for Fabry symptoms to manifest.
Because males only have one X chromosome, the presence of a disease-causing mutation on their GLA gene means they will develop the condition. But women have two X chromosomes, so it’s possible that a healthy copy of GLA on one of the X chromosomes might partially compensate for a mutated copy on the other.
As such, Fabry disease in females is more variable than Fabry disease in males. Indeed, women with a Fabry mutation may be entirely asymptomatic and/or have normal alpha-Gal A activity levels.
This can make it much easier to miss the condition in female patients, but it is still critical that they be promptly and accurately diagnosed. Symptoms may emerge later on, and women can pass the disease to their future children. Genetic testing for Fabry is critical for women who have a family history of disease, even if they don’t have any signs of it.
In children, early signs of Fabry may be subtle and easily missed. For example, children may find it harder to exercise relative to their peers because of heat intolerance and fatigue, but this might not always be noticed as a medical issue.
Fabry disease may also be confused with other pediatric conditions, such as juvenile arthritis, growing pains, or rheumatic fever, but careful clinical evaluations can help doctors make the right diagnosis.
Fabry Disease News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related articles
-
-

-
-
 Discussion
Discussion
-
 Discussion
Discussion
-
